Text size
Line height
Text spacing

IVF began more than 40 years ago, and since that time it is estimated that more than 8 million people have been born from pairs who needed ART techniques to conceive. Originally ART was used as a therapeutic treatment for infertile couples with irreversible tubal factor infertility, but gradually it has been extended to situations of infertility caused by other factors (such as male factor, endometriosis, PCOS; or other types of unexplained infertility). Moreover, impaired reproductive capacity of a people, such as single women, same-sex couples has been also addressed from ART. Because of the many political, social, and sensitive ethical issues surrounding ART practice, it is not unexpected that different regulations exist in different countries. To date there are no consensus based regulatory measures in Europe. Regulations differ from country to country thus the availability of ART for individuals, the method, costs, possibility of preimplantation diagnostic, availability of counseling vary.
Many factors have been examined and recognized as contributing to these very important differences between countries. Some relate to financial issues such as affordability, cost of treatment, and user co-payments. Others relate to cultural and belief dimensions (religious patterns of the community or level of acceptance by society). Some differences root from long existing political traditions, which deeply influence policy making.
Slide 3 Europeans is still have divided opinions about the assessment of ART
An online poll of 6,000 people covering France, Germany, Italy, Spain, Sweden, and the UK shows that Europe is still divided in its assessment of assisted reproductive technologies (ART) (Fauser et al., 2019). A majority of 54% of the respondents across all these countries was positive about IVF. But there was also a strong minority of skeptics: 46% of the respondents agreed to the statement they “never had, nor would (…) ever consider IVF treatment”. There was also variation in public attitudes between countries. There was a majority of skeptics in France and Germany (62% and 57%, respectively); Opponents were a strong minority in the UK (46%); Large groups of people were skeptical of ART in Sweden (39%), Italy and Spain (38%). Fauser et al. (2019)
Slide 4-5
A number of questions arise as a result of the aspects mentioned above.
Legal framework
Most countries reported having specific ART laws, in which various ART techniques are precisely regulated, but these laws differ from country to country. ART methods include in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), preimplantation genetic diagnosis (PGD), preimplantation genetic screening (PGS) as well as egg donation, sperm donation, embryo donation, surrogacy.
No regulating law exists in Albania, Bosnia and Herzegovina (Federation), Ireland, Romania and Ukraine.
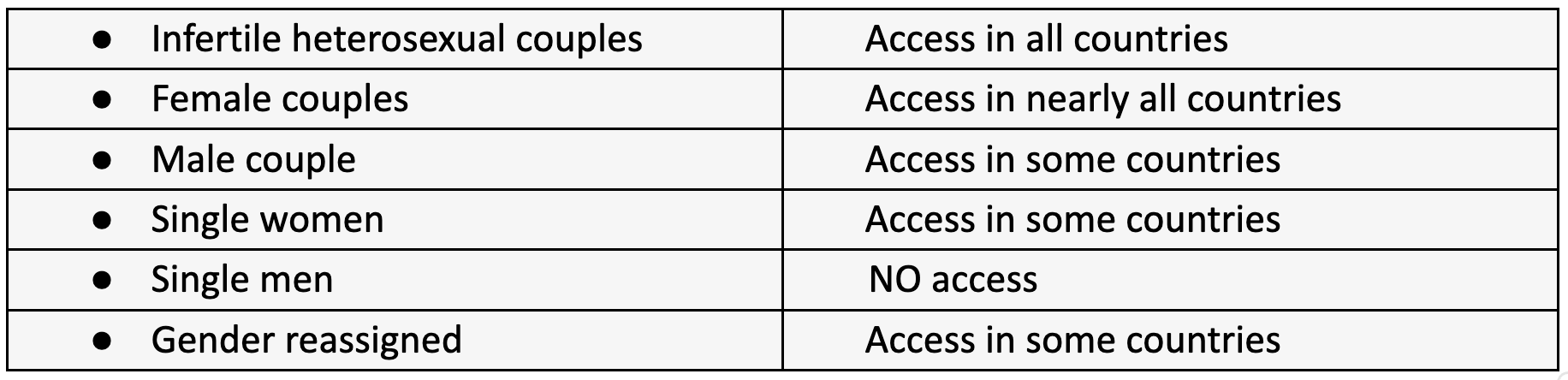
But these laws also make a strict distinction as to who has access to these ART techniques.
Access is restricted by law to heterosexual couples in 11 countries – Albania, Bosnia and Herzegovina, Czech Republic, France, Italy. Lithuania, Poland, Slovakia, Slovenia, Switzerland and Turkey. In Romania, the Netherlands and Uk, as well as Belgium and Malta, ART and IUI techniques are also allowed for single women and same-sex couples. Most countries fall somewhere between these two extremes, with a total of 30 where treatments are available for single women and 18 countries where treatments are also available for female couples. A transgender person can have access to ART techniques in 21 countries.
IUI counts as an ART technique under the national laws of 35 countries.
The use of donated sperm in ART and IUI is legal in most countries except Bosnia and Herzegovina and Turkey. However, Croatia and Montenegro indicated that local donors are not available in their countries, which is why sperm can only be imported to Croatia from abroad. Multaneous donation of sperm and egg is not permitted.
Egg donation is not allowed in Bosnia and Herzegovina, Germany, Norway, Switzerland and Turkey. Although accepted in Croatia, Ireland, Italy and Montenegro, no local donations are made.
Simultaneous sperm and egg donation is not allowed in countries where egg donation is banned, such as Armenia, Croatia, France, Montenegro, Slovenia and Sweden. 14 countries do not allow embryo donation, including Austria, Armenia, Belarus, Bosnia and Herzegovina, Bulgaria, Denmark, Iceland, Italy, Kazakhstan, Norway, Slovenia, Sweden, Switzerland and Turkey.
In some countries there is also a difference in relation to certain techniques. This is the case for preimplantation genetic testing (PGT) for monogenic diseases/chromosomal structural changes (PGT-M/SR; formerly PGD), which is allowed in all countries except Bosnia and Herzegovina and Malta.
PGT for aneuploidy (PGT-A; formerly Preimplantation Genetic Screening) is not allowed in Bosnia and Herzegovina and Malta, as well as in Denmark, France, Germany, Hungary, Lithuania, Norway, Slovenia, Sweden and the Netherlands.
Surrogacy is legal in Albania, Armenia, Belarus, Belgium, Cyprus, Czech Republic, Georgia, Greece, Kazakhstan, Macedonia, Romania, Russia, Netherlands, United Kingdom and Ukraine.
Embryo sex selection (with the exception of PGT-M for sex-linked diseases) is not allowed in any of the 43 countries.
Situation worldwide:

Legal limits for ART access
As previously mentioned, marital status and sexual orientation are often considered limitations on ART. However, 34 of the 43 countries also have legal age limits for candidates for ART. In 21 countries, men and women must be over 18 years of age. Belgium, Kazakhstan and Malta define a minimum age for women but have no such restriction for men. The maximum female age is also a legal limit in 18 countries, ranging from 45 years in Denmark and Belgium (in the latter this limit applies to egg retrieval, while embryo replacement and insemination are allowed up to 47 years) to 51 in Bulgaria. In Austria, "natural cycle available" is an undefined criterion for a maximum age until women reach menopause. The maximum age for men is 60 years in Portugal, while in Finland 60 years and in Sweden 56 years are recommended age limits for men. According to Swiss regulations, "the potential father should be able to live until the child is 18 years old". A particular case is France, where there is no definition of numerical age limits and it is the responsibility of the centers to define the legal notion of “normal reproductive age” in practice.
It is also interesting to mention that in Lithuania, for example, ART is not allowed if patients have medical contraindications listed in the specific ART law. According to the regulations in Germany, ART is not reimbursed after sterilizations such as vasectomy and tubal ligation.
Legal limits in third-party donations
Sperm donation is restricted to men over the age of 18 in 16 of the 41 countries where donation is legal. In other countries where the procedure is allowed, no minimum age is defined. 21 countries have maximum male ages for donors, ranging from 35 in Hungary, Kazakhstan, Russia and Slovakia to 55 in Slovenia. The most common maximum age is 40 years. In 30 countries there are some restrictions on the number of infants from the same donor, although in five countries this restriction is only a recommendation and not a legal obligation. This number ranges from 1 Cyprus to 25 in the Netherlands. In 7 of the 30 countries (Belgium, Denmark, Finland, Portugal, Slovenia, Sweden and United Kingdom) there is a maximum number of families/women who can have children from the same donor (from two for Slovenia to 12 for Denmark).
Egg donors must be over 18 in 15 of the 36 countries where donation takes place. 25 countries set a maximum age for donors, ranging from 34 in Serbia to 38 in France, with the vast majority of countries setting the limit at 35. Bulgaria and Denmark have less restrictions on the maximum age of the donor if the donors/relatives are known to each other. In Belarus, Bulgaria, Hungary and Ukraine, egg donors must have at least one child. This condition is considered desirable but not mandatory when selecting egg donors in Romania and Sweden. The maximum number of donations is set in 10 countries - from one (two in rare exceptions) in Slovenia to 20 in Belarus. The most common numbers are between 4 and 6. 25 countries have defined a maximum number of infants from the same donor, although in 3 of them it is only a recommendation and not a legal requirement. This value ranges from 2 in Montenegro to 10 in France, Greece, Kazakhstan and Italy. In 6 of the 25 countries (Belgium, Finland, Serbia, Slovenia, Sweden and the UK) there is a maximum number of families/women that can have children from the same egg donation (from 1 for Serbia to 10 for the UK). Armenia, Bosnia and Herzegovina, Germany, Iceland, Ireland, Moldova, Poland, Republic of Serbia, Russia and Turkey don’t have legal age limits for ART. In other countries, such as Switzerland, the age restrictions are not clearly declared.
There is no embryo donation in Austria, Armenia, Belarus, Bulgaria, Denmark, Iceland, Italy, Kazakhstan, Slovenia, Sweden and Switzerland.
The issue of anonymity
There are different approaches to anonymity of the donors across Europe.
Regarding gamete donation, four different scenarios were identified. Strict anonymity is the rule in 18 countries, although 5 of these countries allow disclosure of the donor's identity in the event of serious health problems of the child. A special situation is Lithuania, where the identity of a donor may be known after a court decision for other (unspecified) important reasons. In some countries (Estonia, Poland and Russia) general information about the donors (nationality, age, weight, height, education) is available for recipients and children. In a second group of countries, the recipients are anonymous, but the children born can have access to the donor's identity if they are over a certain age (Austria, Croatia, Finland, Malta, Portugal, United Kingdom). A third scenario is gamete donation in a mixed system (anonymous and non-anonymous) as described in 13 countries. In Bulgaria, non-anonymity is an exception and affects donors who are relatives, while recipients in Germany and Switzerland can bring their own donor who will only donate to that couple. In Belgium, non-anonymous donation is only allowed if there is a formal agreement between the donor and the recipient. Georgia, Romania and the Netherlands are countries with non-anonymous embryo donation, while in Georgia and the Netherlands this also applies to gamete donation. In Hungary, egg donors must be a relative of the recipient, but a sperm donor must be anonymous. While local donations in Romania do not have to be anonymous, imported gamete donations can also come from anonymous donors. Whereas in Georgia and the Netherlands, non-anonymity is the rule for gamete donations.
Embryo donation is allowed in 29 countries under one of three perspectives: strict anonymity, anonymity except for born children, and non-anonymity. No country has a mixed system of embryo donation. Five of the 13 countries with a mixed situation for gamete donation allow embryo donation under strict anonymity (Belgium, Germany, Hungary, Ireland and Ukraine). In Romania embryo donation is possible only with non-anonymous donors, while in the seven remaining countries Embryo donation is not performed.
Preservation of fertility potential
Fertility protection, gamete cryopreservation for fertility-limiting diseases is allowed in all countries, although 17 of them have no specific legislation. The same applies to the cryopreservation of gonad tissue (with the exception of Bosnia and Herzegovina, where the technique is not performed). The cryopreservation of embryos for medical reasons is not permitted in Italy and Portugal, but is only possible in Germany in the two-nuclear stage and is carried out in all other countries. Non-medical egg freezing is not allowed in Austria, France, Hungary, Lithuania, Malta, Norway, Serbia and Slovenia, nor is it performed in Bosnia and Herzegovina and Moldova, although there are no laws prohibiting this technique.
Non-medical egg freezing /social freezing (which countries allowed?)
Public Funding
The importance of public and private ART centers varies greatly from country to country.
In 29 of the 39 countries with public financial support for ART, access to public funding is subject to some limiting criteria, such as the age of the woman or man, the indication, the number of previous attempts, or the presence of previous children.
In order to contract with the public support system, centers in Austria, Bulgaria, Finland, Romania and the United Kingdom must have a minimum success rate. A special case is Hungary, where no minimum success rate is required, but public centers receive a special amount of money for each live birth resulting from ART.
The total number of cycles reimbursed also varies by country, with information on some countries requiring additional detail. In Austria, for example, the funded number of cycles per clinical pregnancy applies without a defined limit on the number of pregnancies.
In 19 countries, not all ART performed are eligible for public financial support. PGT is not promoted in Bulgaria, Greece and Italy. Russia and Spain (Spain is not supported only for repeated implantation failures). Expenditure related to donor cycles is not financially supported in Estonia, Montenegro and Russia. Cryopreservation of gametes and embryos is not publicly funded in the Czech Republic, Lithuania, Montenegro and Russia. In the case of premature ovarian failure, egg donation is not publicly supported in Spain for women over 36 years of age. Iceland and Ukraine indicated that only standard IVF/ICSI receive public funding, and the Czech Republic and Slovakia maintain that there is no public financial support for ICSI. Austria, Latvia and Turkey, "add-on" techniques are not included in the public funding. The Federation of Bosnia and Herzegovina, Macedonia and the United Kingdom indicated that not all techniques will be funded, but no details were given.
In Belarus, the Federation of Bosnia and Herzegovina, Estonia, Denmark, Germany, Italy, Kazakhstan, Norway, Russia, Spain and the UK, ART was considered to be unequally publicly funded across the country.
So there are lots of points to be debated
-> Difference in regulations lead to „Fertility Tourism“
Fertility Tourism
Over 97% of infertile couples are actively considering the concept of a fertility journey.
Cost does not appear to be the primary reason for all travelers, with the possible exception of younger patients who do not have comparable access to financial resources as their older counterparts.
Surprisingly, providing anonymous donors isn't the main determinant of the fertility traveler either — although it is important for some. It is much more the possibility of different treatments and feedback from patients who have returned from treatment.
Recently, more fertility clinics have opened in different places and the fertility tourists are overloaded with the number of choices. Countries that have traditionally done well in treating international patients continue to do so - Spain, Greece and Cyprus remain popular, but new markets such as the Czech Republic and Ukraine are becoming increasingly popular. At the moment the war in Ukraine forced fertility centers to reduce or stop their current activites.
Efficient and reliable regulatory frameworks are also important drivers for patients and this is a reason for patients to seek treatment in countries like the United States and the United Kingdom. Visitors to treatment providers in these countries are not necessarily driven by price but by the reassurance and perception that they are receiving quality, regulated treatment that is performed professionally.
Yet there is no such thing as a general fertility tourist. Everyone has a different portfolio of needs, demands, expectations, doubts and fears and must be treated as an individual.
Nevertheless, the worries that torment patient couples,- be it the language barrier, travel arrangements or the legal framework- should not be ignored.
Europe moves towards complete statutory regulation of assisted reproduction. But large variations still exist in how the legislation is applied. So what are the real questions behind the legal regulation and practice of assisted reproductive technology?
Fauser et al. (2019): Beliefs, attitudes and funding of assisted reproductive techNeinloigies. Public perception of over 6,000 respondents from 6 European countries. PLOS One, 14(1).)
C. Calhaz-Jorge, Ch De Geyter, M.S. Kupka, C. Wyns, E. Mocanu, T. Motrenko, G. Scaravelli, J. Smeenk, S. Vidakovic, and V. Goossens. "Survey on ART and IUI: legislation, regulation, funding and registries in European countries ." Human Reproduction Open 2020: 1-15.
Fincham, Anita. fertility europe. 10 December 2021. 08 December 2022. <https://fertilityeurope.eu/european-atlas-of-fertility-treatment-policies/>;.
European IVF-monitoring Consortium. ESHRE. 31 December 2020. 08 December 2022. <https://cm.eshre.eu/cmCountryMap/home/index/2021>;.



